


1Department of Dermatology and Allergy, Ludwig Maximilian University, Frauenlobstr. 9-11, DE-80337 Munich, 2Department of Human Genetics and 3Department of Dermatology, University Medical Center Regensburg, Regensburg, and 4Department of Human Genetics, Medical Center – University of Freiburg, Faculty of Medicine, University of Freiburg, Germany. *E-mail: Andreas.Wollenberg@med.uni-muenchen.de
Accepted Nov 20, 2018; E-published Nov 21, 2018
Dorfman-Chanarin syndrome (DCS), known as neutral lipid storage disease with ichthyosis, is an autosomal recessive disorder caused by mutations in the ABHD5 gene responsible for triglyceride degradation (1, 2). Lipid droplets accumulate in various cells, including granulocytes, keratinocytes, hepatocytes, Schwann cells and epidermal Langerhans cells (3). Currently, there is no treatment for DCS and the management of symptoms and potential complications requires multidisciplinary coordination.
Skin involvement is characterized by ichthyosiform non-bullous erythroderma, and adequate treatment poses a challenge to dermatologists. Various topical therapies, including emollients and keratolytic agents, have been proposed to improve ichthyosis, with mostly unsatisfactory results (4). While systemic therapy with retinoids has been used successfully in patients with ichthyosis, co-morbidities limit its use in DCS. We report here overall clinical improvement with local use of tazarotene 0.015% cream in a female patient with DCS manifesting with ichthyosis, hepatomegaly and cataracts.
An 18-year-old woman born to a consanguineous Kurdish family presented with a history of generalized congenital ichthyosis. Previous genetic testing revealed the homozygous mutation c.594dupC (p.Arg199Glnfs*11) in the ABHD5 gene, consistent with DCS (1). Furthermore, pathognomonic lipid droplets were identified in granulocytes by lipid-specific blood smear coloration.
Topical therapy was initiated with tazarotene 0.015% cream (15 g tazarotene 0.1%, Zorac®, EMRA-MED Arzneimittel GmbH (Trittau, Germany), diluted in 100 g cream base) on the face and left side of the body once daily. The patient was informed about the teratogenic potential of retinoids, and contraception during treatment was advised. As an internal control, the other half of the patient’s body was treated with emollient containing 10% urea in the same vehicle as the diluted tazarotene cream. The treatment was not blinded. Blood samples were taken prior to and 8 weeks after treatment. The liver enzymes, which were elevated prior to therapy, remained stable with no further increase.
After 8 weeks, a clear delineation of the side treated with tazarotene 0.015% was evident. The left side had significantly less scaling than the right side treated with 10% urea, where skin findings were similar to baseline, and the patient observed sweating on the left side of her body (Fig. 1e).
To assess these findings, transepidermal water loss (TEWL) was measured using TEWAMETER TM210® and stratum corneum hydration (SCH) using Corneometer®825 at baseline and 8 weeks after therapy. An increase in TEWL is seen in patients with a disrupted skin barrier, indicating increased water loss and decreased hydration of stratum corneum (4). The side treated with tazarotene showed lower TEWL and higher SCH values than the side treated with urea 10%, indicating overall improvement in skin barrier function following tazarotene treatment (Table SI).
Optical coherence tomography (OCT), a non-invasive method to examine skin changes, was performed at baseline and after 8 weeks using VivoSight OCT®, Firma Michelson Diagnostics Deutschland GmbH (Schwarzenbruck-Altenthann, Germany), which allows an imaging depth of approximately 1.5–2 mm (5). A coherent interpretation of the OCT image was performed by using histopathological images from a previous biopsy as a template. At baseline, OCT identified an abnormal hyper-reflective stratum corneum indicative of hyperkeratosis, an increased epidermal thickness, a thinned granular layer and papillomatosis, all consistent with the histopathology. Following treatment, OCT showed an absence of scales, normalization of the epidermal thickness and of the granular layers (Fig. 1a, b). The epidermal thickness decreased from 0.2094 ± 0.03560 mm to 0.1508 ± 0.03121 mm after 8 weeks of therapy (p < 0.0001) (6).
After 8 weeks, urea 10% was stopped and tazarotene 0.015% cream was applied to the whole body. Follow-up after 13 months of topical therapy revealed satisfactory clinical improvement.
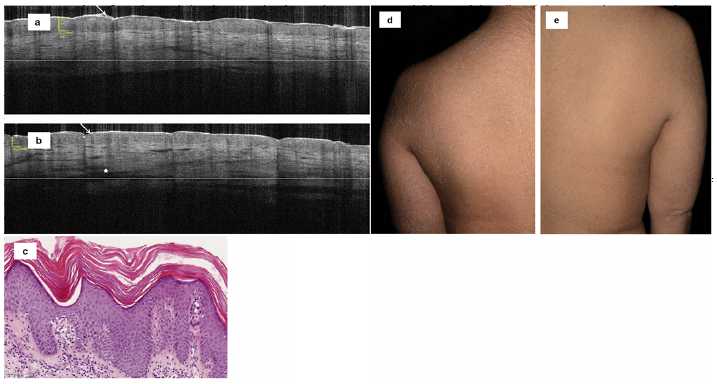
Fig. 1. Forearm of the 18-year-old patient with Dorfman-Chanarin syndrome imaged by optical coherence tomography before: (a) and after 8 weeks (b) of therapy with topical tazarotene 0.015%. (a) Before treatment, hyperkeratosis is visible as an abnormal hyper-reflective stratum corneum (arrow); the epidermal thickness appears to be increased, while the granular layer is thinned. The undulating surface corresponding to the papillary projections of the epidermis indicates papillomatosis. (b) After treatment, absence of scale (arrow) is accompanied by a normalization of the epidermal thickness and the granular layer, together with a flattening of the papillae. Increased dermal vascularization is also present (asterisk). (c) Histological image of skin biopsy before therapy showing epidermal achanthosis and hypergranulosis, (haematoxylin and eosin stain, original magni?cation ×20). (d) Skin findings after 8 weeks of therapy with urea 10% cream. (e) Skin findings after 8 weeks of therapy with tazarotene 0.015% cream.
DCS is a disorder with many systemic implications. The most obvious is physical appearance, since patients have congenital erythrodermic ichthyosis (7, 8). Keratolytic agents were not considered as treatment options for our patient, due to side-effects following systemic absorption. Although the use of systemic retinoids has been reported in individual cases of DCS with satisfactory results and tolerability, concerns regarding worsening of the elevated liver enzymes precluded its use (7). Tazarotene is a retinoic acid that has shown favourable results in patients with ichthyosis when used topically in a 0.1% formulation. We diluted tazarotene to 0.015% and tested this formulation on half of the patient’s body. She reported good tolerability, which allowed for full adherence to therapy.
While many authors have published their experience with different types of ichthyosis, this is the first report of topical tazarotene treatment in a patient with DCS (9, 10). Tazarotene is a retinoid that binds selectively to the RARß and RARγ receptors, mostly expressed in the epidermis. The rapid conversion of the hydrophobic prodrug tazarotene to the hydrophilic active metabolite tazarotenic acid ensures a low level of retinoid in the fatty tissue (11). Tazarotene, therefore, has minimal systemic absorption, even if applied to 90% of the skin in a 0.05% or 0.1% concentration (12). This may explain why tazarotene did not influence the liver enzymes of our patient.
According to the European Medicines Agency (EMA), topical tazarotene is contraindicated in pregnant women. A safety time between treatment and pregnancy is not required by EMA (13). These recommendations should be adhered to.
Our patient had lower TEWL and higher SCH values on the side treated with tazarotene, objectively showing a positive effect on the skin barrier. These changes were captured using OCT imaging pre- and post-therapy. The normalization of the epidermal thickness, thickness of the granular layer and flattening of the papillae layer may be a result of the antiproliferative potency of topical retinoids.
We propose tazarotene 0.015% cream as a potential topical agent for patients with ichthyosis, including patients with DCS with systemic involvement. A larger cohort of patients is required to confirm the beneficial effects of tazarotene and to monitor possible long-term side-effects.
This work has been supported by the Deutsche Stiftung Kinderdermatologie.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize